Told You Need a Knee Replacement?
You May Have More Options Than You Think.
This guide covers every treatment for bone-on-bone knee pain — from conservative therapy to surgery — so you can make an informed decision backed by 40,000+ patient outcomes.
*Based on 400K+ actual patient billing records at Joint Relief Institute. Individual costs vary.
What “Bone-on-Bone” Really Means
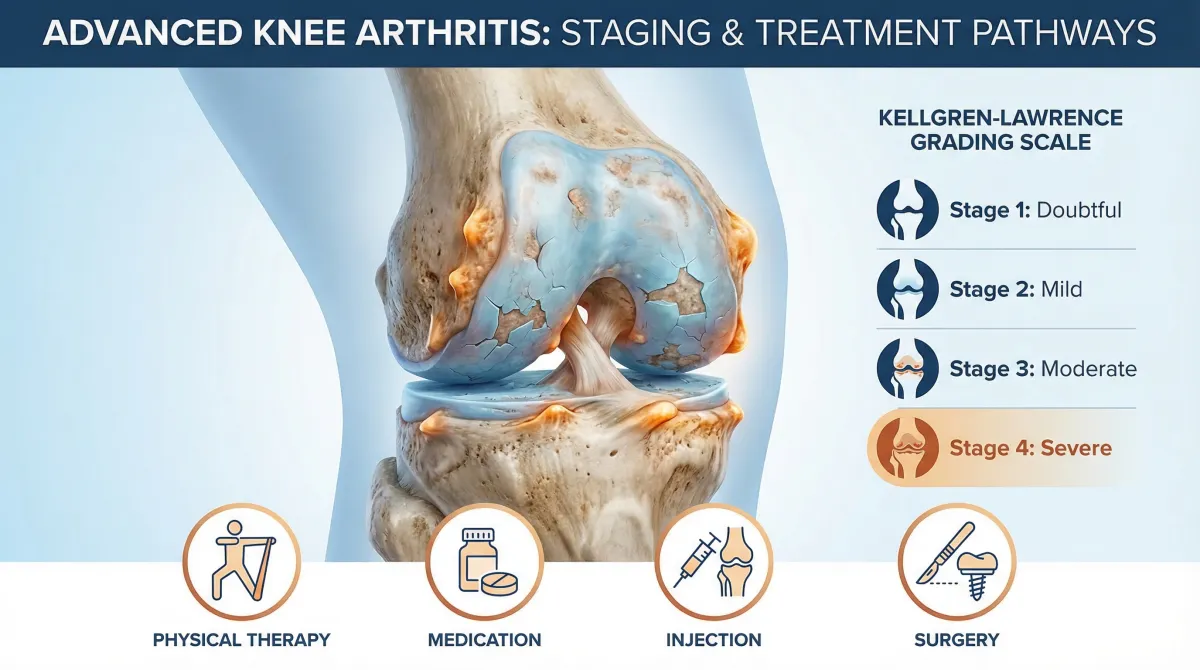
Not all bone-on-bone knees are the same. The Kellgren-Lawrence scale classifies arthritis severity from 0 to 4. Many patients told they're “bone-on-bone” are actually Grade 3 — where significant cartilage still remains and non-surgical treatment is highly effective.
Grade 0: Normal
Healthy knee with intact cartilage. No treatment needed.
Cartilage: Full thickness
Grade 1: Doubtful
Minor wear with possible small bone spurs. Mild stiffness.
Cartilage: Minimal thinning
Grade 2: Mild
Definite bone spurs visible. Joint space beginning to narrow.
Cartilage: Noticeable thinning
Grade 3: Moderate
Multiple bone spurs. Definite joint space narrowing. Sclerosis present.
Cartilage: Significant loss
Grade 4: Severe
Large bone spurs. Severe narrowing. Bone-on-bone contact.
Cartilage: Near-complete loss
Key insight: The right treatment depends entirely on your KL grade. An evaluation with imaging is the only way to know your exact severity level. Many patients are surprised to learn they have more options than they were told.
Every Treatment Option, Ranked
From least invasive to most invasive. Start with conservative options and escalate only as needed.
Physical Therapy & Exercise
Strengthens muscles around the knee to reduce load on the joint. Improves range of motion and flexibility.
Advantages
- No risk
- Improves overall fitness
- Can be combined with any treatment
Limitations
- Requires consistent effort
- Limited relief for severe arthritis
- Does not restore cartilage
Oral Medications (NSAIDs)
Anti-inflammatory drugs reduce swelling and pain. Includes ibuprofen, naproxen, and prescription options.
Advantages
- Fast-acting
- Widely available
- Low cost
Limitations
- Stomach/kidney risks with long-term use
- Masks pain without treating cause
- Diminishing returns
Cortisone Injections
Corticosteroid injected into the joint suppresses inflammation and provides fast pain relief.
Advantages
- Fast relief (2–3 days)
- Low cost
- Good for acute flare-ups
Limitations
- Short-lasting
- May accelerate cartilage damage with repeated use
- Limited to 3–4 per year
Gel Injections (Viscosupplementation)
JRI SpecialtyHyaluronic acid injected into the joint restores lubrication and cushioning. Reduces bone-on-bone friction. At JRI, gel is typically combined with cortisone for faster onset of relief.
Advantages
- Long-lasting (6+ months)
- May protect remaining cartilage
- Repeatable every 6 months
- No surgery recovery
- Can combine with cortisone for immediate + lasting relief
Limitations
- Gradual onset (1–2 weeks)
- Requires fluoroscopy for best results
- Less effective at KL 4 without repeated courses
Knee Bracing & Offloading
Unloader braces shift weight away from the damaged compartment of the knee, reducing pressure on affected areas.
Advantages
- Non-invasive
- Immediate relief while worn
- Can combine with other treatments
Limitations
- Bulky
- Only helps while wearing
- Does not address underlying condition
Partial Knee Replacement
Replaces only the damaged portion of the knee. Preserves healthy bone and ligaments.
Advantages
- Preserves healthy tissue
- Faster recovery than total replacement
- More natural-feeling knee
Limitations
- Still surgery with risks
- 4–6 week recovery
- May need total replacement later
Total Knee Replacement
Damaged bone and cartilage are removed and replaced with metal and plastic components.
Advantages
- Definitive solution for end-stage OA
- Long-lasting
- Proven surgical procedure
Limitations
- 3–6 month recovery
- Surgical risks (infection, blood clots)
- Permanent and irreversible
- 15% need revision within 20 years
The Best Middle Ground for Most Bone-on-Bone Patients
Gel injections occupy a unique position: more effective than conservative therapies, far less risky than surgery. For patients with KL Grade 2–4 arthritis, they offer meaningful relief without the trade-offs of a major operation.
6+ Months of Relief Per Course
Outlasts cortisone by 3–4x. Cumulative improvement with each series.
May Protect Remaining Cartilage
Unlike cortisone (which can accelerate cartilage loss), hyaluronic acid may have chondroprotective properties.
Zero Recovery Time
Walk out the same day. No hospital, no rehab, no time off work.
Medicare-Covered
Most qualifying patients pay little to nothing out of pocket.
Patient Satisfaction Rate
Multi-practice study of 782 patients over 6 years
Why Fluoroscopy Matters More for Bone-on-Bone Knees
In severely arthritic knees, the joint space may be just millimeters wide. Blind injections miss this target up to 30% of the time. At JRI, every injection is fluoroscopy-guided for 100% accurate placement.
Up to 30% of injections miss the joint entirely
Real-time X-ray confirms every injection reaches the joint
Why this matters for bone-on-bone knees: When the joint space is severely narrowed, precision is everything. A missed injection means wasted time and medication. Fluoroscopy eliminates guesswork.
When Surgery IS the Right Answer
We believe in honest recommendations. At JRI, we refer patients to surgery when it's genuinely the best path — even though it means we're not the ones providing the treatment.
Surgery may be best if:
Multiple courses of gel injections have provided diminishing returns
Pain significantly limits basic daily functions like walking and standing
Structural joint damage is too severe for conservative treatment to address
Your quality of life would clearly be better served by surgical intervention
Your overall health supports surgical recovery (no major complications risk)
Important: Trying gel injections first doesn't mean choosing instead of surgery. It means exploring a low-risk option that may provide years of relief before surgery becomes necessary. And if you do eventually need a replacement, you'll have maintained better joint function and fitness in the meantime.
What Our Bone-on-Bone Patients Say
“My surgeon said I was bone-on-bone and needed a replacement. I tried gel injections first — that was 4 years ago. I’m still walking my dog every morning.”
“I have Grade 3 arthritis in both knees. After three rounds of gel injections, I’m back to gardening and playing with my grandkids.”
“I was told surgery was my only option. Joint Relief Institute was honest — they said gel injections could help but might not be permanent. Three years later, I’m grateful I tried.”
More Patient Experiences
My knees feel wonderful and brand new after my injections. I was scared of surgery but this worked beautifully.
My sister got relief with just 3 injections — no surgery needed! Anybody with knee pain, I recommend here. Now I'm ready for my cruise!
I wish that I had gone to them earlier. They told me exactly what my Medicare would cover. Courteous, concerned, and highly professional.
5 Convenient Locations
Chicagoland clinics in Glenview, Oak Brook, Orland Park, and Stony Island — plus our Minneapolis-area clinic in Edina, MN.
Every Month You Wait, Cartilage Continues to Wear Down
Gel injections work best when there's still cartilage to protect. The earlier you start, the better your long-term outcomes.
Check Your Insurance Coverage
Medicare and most insurance plans accepted
Frequently Asked Questions
Q1. What does "bone-on-bone" actually mean?
Bone-on-bone describes advanced knee osteoarthritis where cartilage has worn away significantly, allowing bones to make direct contact during movement. The medical classification uses the Kellgren-Lawrence scale (grades 0–4). Many patients told they are "bone-on-bone" are actually Grade 3 (moderate) rather than Grade 4 (severe), which affects treatment options significantly.
Q2. Can you avoid knee replacement with bone-on-bone arthritis?
Many patients with bone-on-bone arthritis successfully delay or avoid knee replacement through non-surgical treatments like viscosupplementation (gel injections). Clinical data shows 88.7% patient satisfaction with gel injection therapy, and patients who commit to repeated courses every 6 months often experience progressive improvement. However, some patients with the most severe joint damage may eventually benefit from surgical intervention.
Q3. Do gel injections work for bone-on-bone knees?
Yes, for many patients. Studies show 38% improvement after a single course and up to 66% improvement after multiple courses. The key factors are accurate injection placement (fluoroscopy guidance), treatment consistency (every 6 months), and realistic expectations.
Q4. What is the best non-surgical treatment for bone-on-bone knees?
The most effective non-surgical approach is typically a combination of viscosupplementation (gel injections) for direct joint cushioning, physical therapy for muscle support, and lifestyle modifications. Gel injections provide the longest-lasting per-treatment relief (6+ months) among non-surgical options and are covered by Medicare for qualifying patients.
Q5. Does Medicare cover treatment for bone-on-bone knees?
Yes. Medicare Part B covers viscosupplementation (gel injections) for qualifying patients with documented knee osteoarthritis who have tried at least 3 months of conservative treatment. Most patients pay only the 20% coinsurance. Call (800) 238-9307 to verify your specific coverage.
Q6. How do I know which Kellgren-Lawrence grade I am?
Your grade is determined by X-ray imaging of your knee joint. During a consultation at Joint Relief Institute, our physicians review your imaging to determine your exact KL grade, which directly informs which treatments are most likely to help. If you have recent X-rays, bring them to your appointment.
Q7. When should I consider knee replacement surgery?
Surgery may be the best option when: non-surgical treatments have been tried consistently and no longer provide adequate relief, your quality of life is severely limited despite treatment, and your overall health supports surgical recovery. At JRI, we recommend surgery when it is genuinely the best path — even though it means referring you elsewhere.
Q8. What is fluoroscopy and why does it matter?
Fluoroscopy is real-time X-ray imaging used to guide the injection needle precisely into the joint space. In bone-on-bone knees, the joint space is extremely narrow, making accurate placement critical. Studies show blind (unguided) injections miss the joint up to 30% of the time. JRI uses fluoroscopy for every injection to ensure 100% accuracy.
Find Out What's Right for Your Knees
The best treatment depends on your specific severity level. Our board-certified physicians will evaluate your imaging, determine your KL grade, and recommend the approach most likely to help.
If gel injections aren't the right fit, we'll tell you honestly — and help you find the specialist who can.
Or call us: (800) 238-9307
Sources
[1] Kellgren JH, Lawrence JS. Radiological assessment of osteo-arthrosis. Annals of the Rheumatic Diseases, 1957.
[2] Long-Term Outcomes of Single versus Multiple Courses of Viscosupplementation. PMC, 2021.
[3] EUROVISCO Consensus Guidelines for HA Viscosupplementation in Knee OA. J Orthopaedic Surgery and Research, 2024.
[4] Accuracy of Blind vs. Image-Guided Intra-Articular Knee Injections. J Clinical Medicine, 2022.
[5] Effect of Intra-articular Triamcinolone vs Saline on Knee Cartilage Volume. JAMA, 2017.
[6] Medicare Coverage Database: Hyaluronic Acid Injections. CMS, 2025.